EuroNews MRPH #15 has been released!
Enjoy the reading!
For better viewing, use the fullscreen mode
Or download it here

EuroNews MRPH #15 has been released!
Enjoy the reading!
For better viewing, use the fullscreen mode
Or download it here
The SAGE Working Group on Vaccine Hesitancy concluded that vaccine hesitancy refers to delay in acceptance or refusal of vaccination despite availability of vaccination services. It is characterized by different factors in different contexts (political, ideological, social, etc.). Vaccine hesitancy is complex and context-specific, varying across time, place and vaccines. [1]
When approaching a hesitant parent, one must never forget that all his doubts are dictated by a strong perception of risk and by the consequent concern for the safety of his offspring. In this context, information concerning the “danger” or the factor considered as such, is connected and elaborated not only at the cortical level, but also in the limbic system which, thanks to its connections with the pre-frontal cortex, comes into play in the decision-making process, based on emotional reactions.
For this reason, any information you want to transmit to the defaulting mother or father, this must be simple, immediate and preferably proposed using the visual means (eg: simple graphs or sample images that can visually reproduce what you intend to explain), according to the rules of cognitive ergonomics. [2]
In the United States in 2010 Dr. Singer developed a communication model that, referring to Aristotelian rhetoric, provides an effective and efficient approach to communicate with the hesitant parents (C.A.S.E. approach). C.A.S.E. is an acronym that identifies the four phases of the communicative approach, Corroborate, About me, Science, Explain / advise (Fig.1). [2,3]
The first phase, Corroboration, which coincides with the Aristotelian technique of pathos, consists in proving emphatic towards parents who do not want to vaccinate their children, that is to listen, welcome and understand their doubts and their fears. Parents must perceive that who they are in front of is not an enemy whose purpose is to oppose them and impose on them a different way of thinking and acting, but it is a person who shares their primary interest, the health of the child. To achieve this, it is very important to find a point of agreement from which to start. [3,4]
In the second phase, About me, or ethos according to Aristotle’s rhetoric, the health worker should explain to parents what is his working mission (e. g. to advance the health of all people, the children’s sake) and what path he has taken to realize it (the studies, conferences or courses in which he participated, various studies). [3,4] The objective is to qualify the speaker, increasing its credibility and making it an authoritative source of information.
The logos of Aristotle is taken up again in the Science phase of Dr. Singer, in which the scientific evidence about the vaccines is presented to the parents. [3,4] It is in this phase when the cognitive ergonomics, mentioned above, comes into play strongly. To make the interview less dispersive, it is advisable for the doctor, already in the corroboration phase, to let the parents express the factors of greatest concern. This on one hand allows to partially reduce the anxiety of mothers and fathers, on the other hand allows the doctor to focus only on some aspects related to the vaccines and not on all the knowledge about the subject.
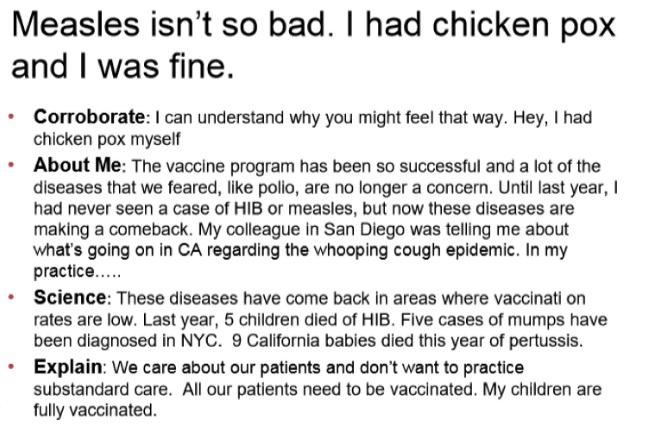
Finally, to conclude the interview, the explain / advise phase should allow to sum up what has been said and give advice to the hesitant parents based on scientific evidence. [4]
The effectiveness of the C.A.S.E. method against hesitant parents has not yet been evaluated in any study. Therefore, assessing effectiveness in the field would be appropriate.
_________________________
References
_________________________
Davide Pezzato
School of Specialization in Hygiene and Preventive Medicine – University of Padua, Italy
Stefania Bellio
School of Specialization in Hygiene and Preventive Medicine – University of Padua, Italy
The access to safe drinking water is essential to health and a basic human right, as well as a structural part of an effective policy for health protection. (1)
Since 1958, aiming primarily to protect public health, the WHO has published several editions of a document, currently called WHO Guidelines for drinking-water quality, which has been regularly updated through rolling revision. This document establishes the principles and guidelines that are the base for the national programs of the United Nations members. (1)
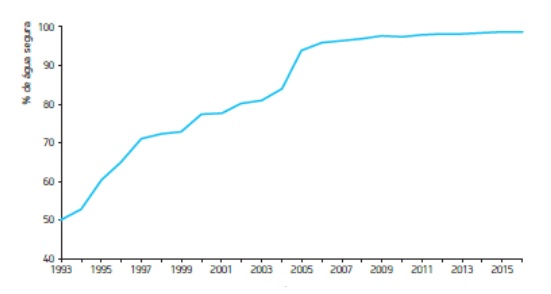
The model for regulating water quality in Portugal has been progressively consolidated through regular legislation revisions that reflect scientific and technical progress. The consequences have been globally positive and are evidenced in a favourable evolution of the indicator on “safe water”, which builds on the fulfilment of sampling frequency and the observance of parametric values (e.g. microbiological and chemical). Figure 1 shows the evolution of the quality level of drinking water; nowadays 99% of water is guaranteed to be controlled and of good quality (in 1993 this indicator was at a mere 50%). (2) (3) (4)
This excellence level is supported by strictly monitoring the stakeholders in this process, among them health authorities that may be integrated in Public Health Units (PHU). (3)
The Activity Plan of the ACeS Alto Ave PHU includes a program of sanitary surveillance for drinking water systems with public distribution. These systems undergo annual characterization as a way to promote risk analysis and management for health. I have recently followed my unit’s environmental health technician on his visits to the drinking water systems in the Fafe area.
These visits started at a Water Treatment Station, where water undergoes a complex treatment process after catchment and is then sent to several reservoirs in the area, which then distribute the water to consumers. Besides verifying the maintenance, hygiene and safety parameters, the process also identifies the treatment types for water (e.g. pre-oxidation, decantation and filtration).
We have then visited all the storage reservoirs in the area where special care is given to the inner lining of tanks/cells, vent protection and latest sanitation date.
Some locations, due to their position and/or demographic rate, benefit from local water capture (e.g. water holes, water springs or wellheads). These Dispersed Systems have their own device for water purification with sodium hypochlorite and sometimes pH correction with caustic soda.

These visits allow us to promote the conservation and maintenance of several infrastructures of the public water supply systems by the appropriate authorities. But they also allow Public Health physicians (as Health Authorities) to intervene in a stricter and more appropriate way in the case of potential infringements of the chemical or microbiological parameters reported. It may therefore be necessary to establish measures to minimize health hazards to the population. (2)
_________________________
References
_________________________
José Miguel Fernandes
Public Health Resident, Public Health Unit ACeS Alto Ave – Fafe
Portugal

Dear friends!
Slovenian public health residents joined EuroNet MRPH in November 2016. Since then we have enjoyed attending every meeting and it is high time for us to organise one ourselves. We hope to take our collaboration to new heights both literally and figuratively. Thus, following on the heels of the EPH Conference in Ljubljana we will be hosting the EuroNet MRPH Winter Meeting on the spectacular alpine plateau of Velika Planina.
Our venue Velika Planina rises to 1,600m offering fantastic views of the surrounding mountains and is just a short drive, cable car and chairlift out of the capital – don’t worry we are organising transport. It is one of the last high alpine herdsmen’s villages in Europe with the plateau dotted with cute wooden huts though we’ll be staying in more comfortable lodgings than the herdsmen of the past (imagine saunas and outdoor wooden hot tubs;). It will be the perfect escape from the city’s public health hazards of noise and air pollution. Enjoying the clean air of the alps and with no distractions around we will be able to focus our energy on networking and the inner workings of EuroNet MRPH.
The General assembly will be hosted at the Zeleni rob restaurant, a snowball’s throw away from the cottages, with plenty of delicious traditional Slovenian food. As public health residents we think we can also be trusted to responsibly enjoy a drink together, just enough to facilitate the exchange of stories from past meetings as well as share our work and new ideas.
A winter fairy-tale is coming and we hope you are going to join us! Don’t forget to apply before October 7th!!
More info at: https://euronetmrph.org/velikaplanina-meeting-2018
Velika Planina, Slovenia 2018
Association of Public Health Residents of Slovenia
Between 2011-2017, pertussis notifications in Ireland were most commonly notified in infants and young children. The age specific incidence rate among the 0-5 month age group peaked in 2012 (ASIR 395/100,000) with smaller peaks in 2016 (235/100,000) and 2017 (225/100,000) Between 2012-2017, of all infant cases, 67% were hospitalised and several infant deaths due to pertussis were notified. None of the mothers of these fatal cases were vaccinated during pregnancy.
Vaccination of pregnant women has been shown to be safe and effective in preventing pertussis in infants. Evidence from data published in England1and Spain2 indicates that protection against pertussis is as high as 90% or more in infants whose mothers were vaccinated in pregnancy.

Antenatal care in Ireland is delivered in three ways: either private care through a maternity unity, free public care through a maternity unit or as free combined care between maternity units and general practitioners (GP). Since 2012, pertussis vaccination in pregnancy has been recommended in Ireland and is available free of charge to maternity units and general practitioners.
However, though the vaccine itself is free, all patients still incur a fee for administration. There is also no clarity or definition regarding where the vaccine should be administered, whether by a GP or in the maternity units. This is thought to contribute to the very low vaccine uptake seen. An audit of maternity units conducted in 2013 showed an uptake rate of 6.2% amongst pregnant women in Ireland. This is far lower than the uptake rate in the UK (73%) where pertussis vaccine is available to pregnant women free of charge.
The lack of a defined pathway for administration and full funding of pertussis vaccination in pregnancy represents a key barrier to increasing uptake. Clarifying a pathway of vaccine delivery and reimbursement should be a priority issue for the Irish health service to ensure that vulnerable infants are protected. Pertussis is a vaccine preventable disease and, as such, every effort should be made to prevent further infant morbidity and mortality.
_________________________
References
1 – https://www.ncbi.nlm.nih.gov/pubmed/25037990
2 – http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=22809
_________________________
Fiona Cianci
Specialist Registrar in Public Health Medicine
Department of Public Health, HSE East, Dublin (Ireland)
I am at the end of the fifth year of the school of Hygiene and Preventive Medicine at the University of Pisa and just before the end I wanted to taste some examples of the best european infection control. Thanks to a precious man, professor Peter Lachman, pediatrician and CEO of the ISQua, I was connected with Haelo that is a quality improvement agency collaborating with many hospitals, one of which is the Salford Royal Hospital. At Haelo they planned for me one-day full immersion on the programs they run routinely with professionals and academics, their methodology and strategies for QI. The next day I was directly into the hospital visiting the amazing A&E Village that is the result of a recent renovation structurally and organizationally: the workflow is designed to let the patient get out of the unit in less than 4 hours unless complications, major injuries or frailty and they normally obtain the >90% patients target! I spent the next days with the Infection Control Team, visiting wards, receiving explanations for every question I posed them, participating to a part of the Induction Package that every new employee must pass before beginning the job. I visited the lab too, talked to a clinical microbiologist about his occupation there and sharing the differences with my country hospital system. I followed a specialist nurse of the IV team in her activity and it was very impressive in matter of competence! Finally two running projects they showed me were the NAAS and CAAS (Nurse and Community Assessment and Accreditation System), examples for how to fix chronic problems like nurses’ professional update and the link between hospital and local health authorities. Outstanding!

Among the other things, have to flag an excellent restaurant inside the hospital, very nice meals consumed during my stay.
Outside I visited the city of Manchester in occasion of the Chinese New Year, the Salford University swimming pool, very nice indeed and the surroundings of Salford, in particular it is worth of remark the most modern area that is MediaCity.
In conclusion, it has been an intense and intensive experience, deep into the world of Infection Control to lean and bring back home a different way to tackle the antimicrobial resistance and the infection transmission in the hospital setting not to mention many ready-to-use tools for my hospital!
_________________________
Giulio Pieve
Public Health Resident, University of Pisa
I’ve been an internal Public Health doctor since January, and I’m taking my first steps in the wide-ranging medical specialty of Public Health. My unit of work covers a wide area including two small-sized cities, Santa Maria da Feira and Arouca, located approximately 40 kms south of Porto. As the first year of an internship in Portugal is focused on Community Health, my daily work is based on 5 major areas: Prevention and Health Promotion, Environmental Health, Health Authority, Epidemiological Surveillance and Health Planning.
In addition to having a particular interest in Global Health, I attend traveller’s consultations in the International Vaccination Center of Porto whenever I possibly can. I grasped the opportunity to attend the World Health Summit Regional Meeting, which took place in Coimbra on the 19th and 20th of April. The congress was held at the San Francisco Convent in a space that gathered around 600 participants and 120 speakers from more than 40 countries to discuss Global Health. A special focus was paid to the health problems faced within countries of the Community of Portuguese Language Countries (CPLC).

Besides the excellent exhibits, interesting debates and networking, which was essential for both professional and personal enrichment, it has also brought many concerns and a feeling that change is essential.
The task of countries considered underdeveloped is increasingly seen as a utopia. The high rates of maternal and child mortality in addition to the high burden of communicable diseases, these countries are facing a growing increase in noncommunicable diseases that until very recently were confined to developed countries. Conversely, developed countries are facing the resurgence of some vaccine preventable communicable diseases, such as Measles in Europe, as a result of a drop in vaccination rates due to the growing anti-vaccine movements we have witnessed. Climate change is a fertile ground for migrations of certain vectors, which may facilitate one of the greatest Public Health problems in countries considered underdeveloped, the vector-borne diseases.
Taking into consideration the future problems resulting from the constant increase of the world population with a prediction of 8.5 billion people in 2030… will there be clean water for all?
We’re a time bomb, and time is counting.
According to various experts in many different areas, even if all efforts were put into practice it would be difficult to achieve the 17 sustainable development goals by 2030. The strategies and measures adopted have been scarce in dealing with the many problems that exist.
We can’t continue to focus solely on the health of our communities, knowing what is happening in the rest of the world.
We can’t all live in Sweden (Ranked 1st the SDG’s rankings), but we can replicate 157 Swedens.
Through the history of Public Health, we have a duty to try to change the world for the better, because anything is possible if someone dreams about it.
_________________________
References
1. World Health Summit Regional Meeting 2018, Coimbra – Portugal. Available: <https://www.worldhealthsummit.org/regional-meeting.html>
2. SDG Index and Dashboards Report 2017 – SGD Index & Dashboards
_________________________
Davy Fernandes
Public Health Resident, Feira-Arouca Public Health Unit, Portugal.